Why Your Neck and Shoulders Hurt — And It’s Not Where You Think
The Thoracic Spine, Distribution of Force, and the Case Against Treating Symptoms in Isolation (7 Mins Read)
Distilled from Polestar Pilates Hour with Brent Anderson, PhD, PT
Most people treat neck pain at the neck and shoulder pain at the shoulder. That’s often exactly why the pain keeps coming back.
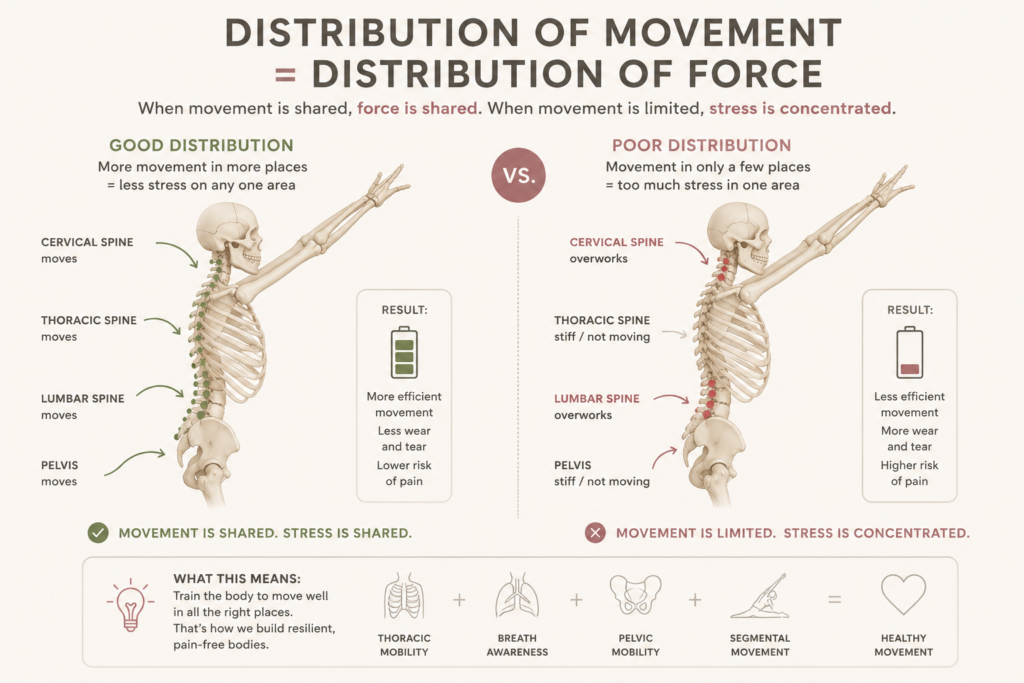
THE PRINCIPLE: DISTRIBUTION OF MOVEMENT = DISTRIBUTION OF FORCE
The thoracic spine — the 12 vertebrae and ribs forming the rib cage — has the greatest movement capacity of any spinal region. In sedentary life, it’s also the region we move least.
When the thoracic spine stops contributing its share of motion, the regions above and below compensate — absorbing force they weren’t built to handle alone. Clinically, this shows up at the lumbosacral junction (L4-5, L5-S1) and the lower cervical spine (C4-5, C5-6) — exactly the segments immediately bordering a stiff thoracic spine.
THE RESEARCH: A 50% DROP IN LUMBAR STRESS, ONE SESSION
A 1996 Loyola Marymount study measured spinal range of motion during forward bending. Nearly all measurable motion came from L4-5, L5-S1 — where most Western low back injuries occur. Thoracic motion was negligible.
After a single 45-minute Pilates reformer session (footwork, bridging, seated roll-down, feet in straps, quadruped), three things changed:
- Overall forward-bending range increased
- Thoracic and upper lumbar mobility increased
- L4-5, L5-S1 force dropped by 50%
The takeaway: it’s not about trunk strength. Increasing thoracic mobility reduces demand at the lumbosacral junction by giving load somewhere else to go — and the same logic applies to the cervical spine and shoulder.
THE RIB CAGE RULE THAT CHANGES YOUR CUEING
Where the spinal disc goes, the rib goes. In extension, the rib moves forward with the disc; in flexion, it moves back. Each rib also follows the transverse process of the vertebra below it — creating a slinky-like opening between ribs during extension.
Without this articulation, all extension force concentrates at one hinge point — the visual you’ve seen countless times: a Swan where the whole rib cage lifts as a rigid block while the low back overworks, or a Roll Up that needs a “thrust” because the lower thoracic isn’t contributing.
Better cue for Roll Up: send the ribs back and underneath the heart, rather than focusing on lifting the legs.
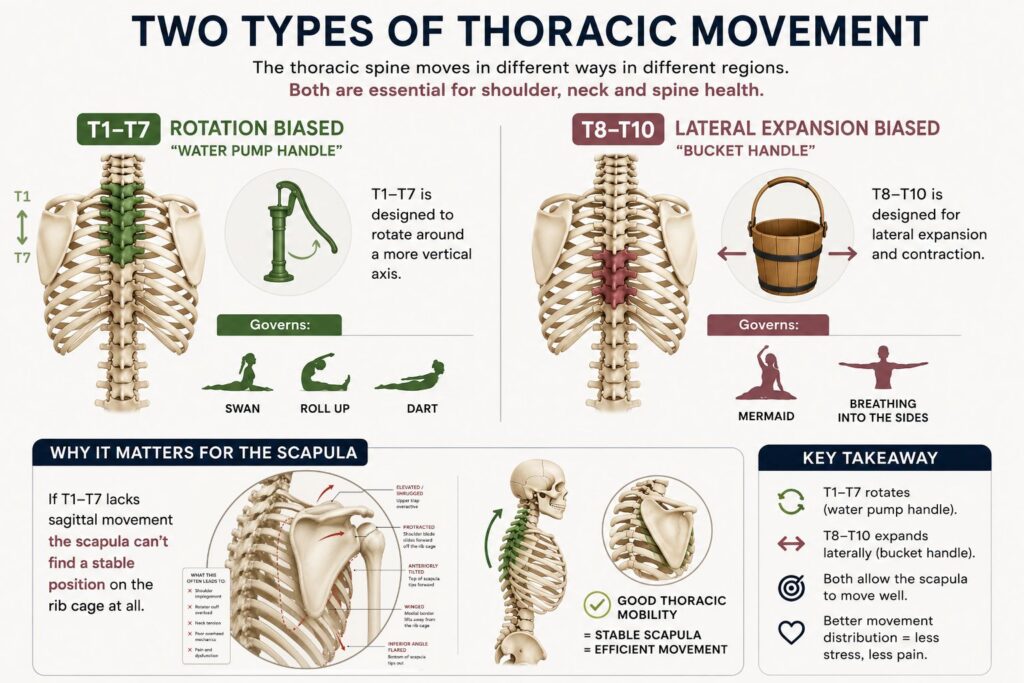
TWO TYPES OF THORACIC MOVEMENT
T1–T7 is biased toward rotation (“water pump handle”) — governs Swan, Roll Up, Dart.
T8–T10 is biased toward lateral expansion (“bucket handle”) — governs Mermaid and breathing-into-the-side work.
If T1-T7 lacks sagittal movement, the scapula can’t find a stable position on the rib cage at all.
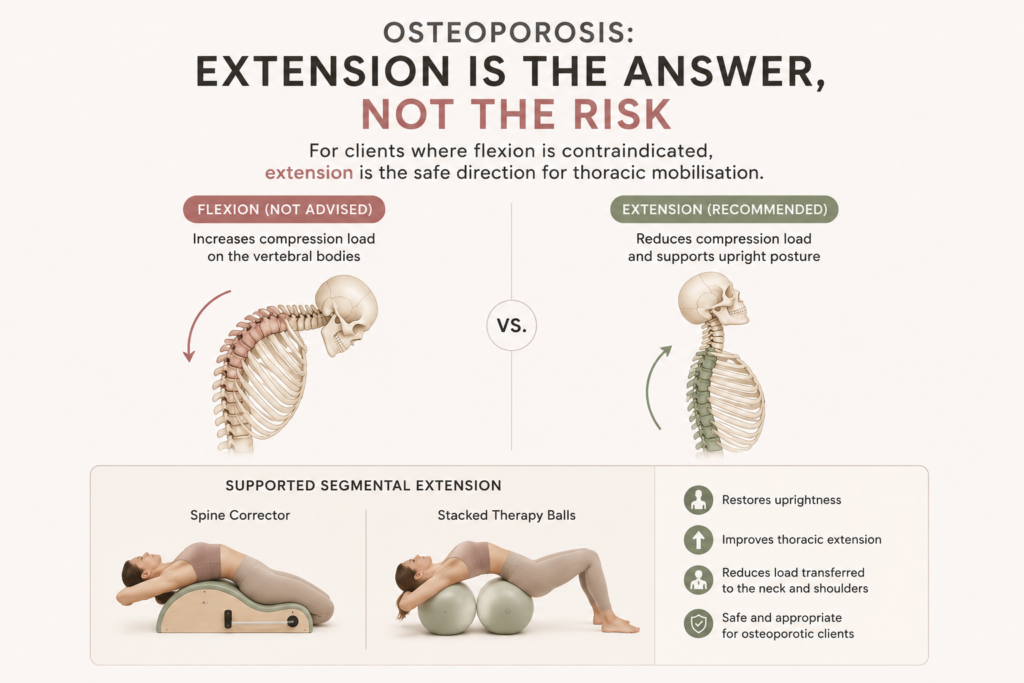
OSTEOPOROSIS: EXTENSION IS THE ANSWER, NOT THE RISK
For clients where flexion is contraindicated, extension is the safe direction for thoracic mobilisation. Supported segmental extension — Spine Corrector, stacked therapy balls — restores uprightness and reduces load transferred to the neck and shoulders.
YOU’RE PROBABLY OVERESTIMATING SEGMENTAL MOVEMENT
Watch a student do Bridge and count the segments that appear to move. Most observers guess 10–12; fluoroscopy often shows 1–2. The fix isn’t more strength — it’s reducing range slightly and repeating, letting the nervous system discover more articulation points.
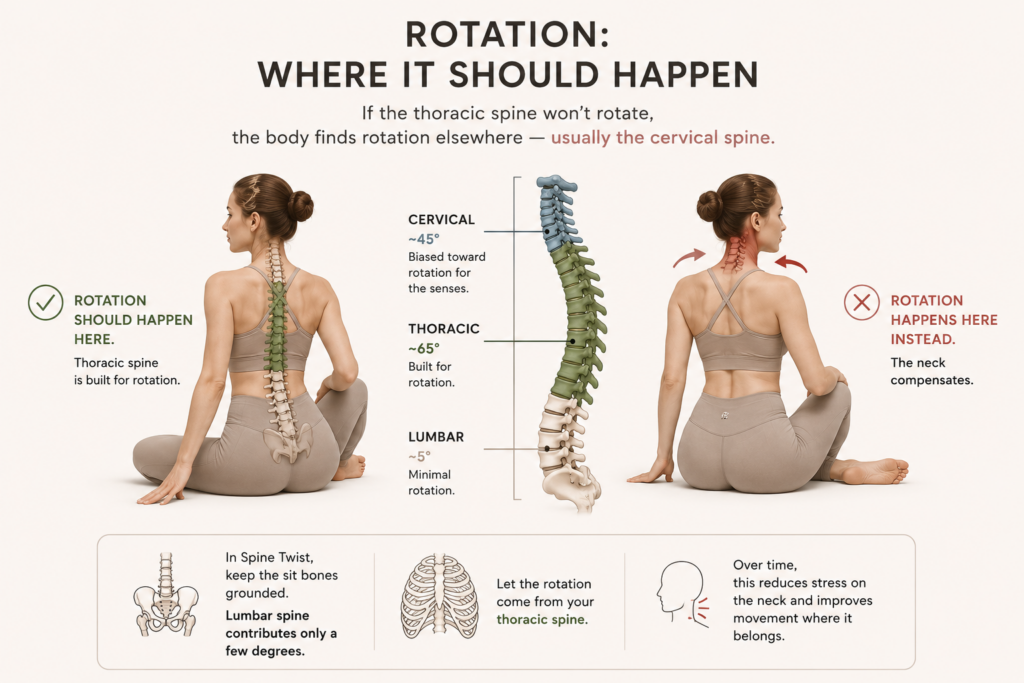
ROTATION: WHERE IT SHOULD HAPPEN
Facet orientation dictates rotation capacity: lumbar facets are sagittal (minimal rotation), thoracic facets sit at ~65° (built for rotation), cervical facets at ~45° (biased toward rotation for the senses).
In Spine Twist, keeping the sit bones grounded isn’t arbitrary — the lumbar spine contributes only a few degrees of rotation per segment. If the thoracic spine won’t rotate, the body finds rotation elsewhere — usually the cervical spine.
THE SHOULDER GIRDLE: WHERE IT ALL CONVERGES
The scapula moves through six motions but cannot extend or horizontally rotate on its own. For any overhead movement — a serve, a reach overhead — the thoracic spine must supply extension and rotation so the scapula stays congruent with the humeral head.
A restricted rib cage that won’t allow the clavicle and scapula full range creates repeated mechanical impingement — the humeral head compressing the rotator cuff tendons with every overhead motion. This is a frequently overlooked mechanical driver of rotator cuff tendinopathy.
WHAT THE PUBLISHED RESEARCH SHOWS
Rotator cuff tear prevalence does rise with age. A 664-subject study found tear prevalence of 10.7% in the 50s, 15.2% in the 60s, 26.5% in the 70s, and 36.6% in the 80s. But asymptomatic tears were roughly twice as common as symptomatic ones from the 60s onward — a tear on imaging isn’t the same as a painful, limiting one. Many older adults with confirmed tears keep playing sport with minimal symptoms.
The “half of people over 50” framing is a reasonable clinical generalisation, not an exact figure — and what’s still genuinely open is how much of this rise is an inevitable biological clock versus decades of force concentrated on two or three overworked segments.
CLINICAL TAKEAWAYS
Osteoporotic clients with neck/shoulder pain: prioritise supported segmental extension.
Rotator cuff tendinopathy: assess thoracic extension and rotation before isolating the shoulder.
Cervical degeneration at C4-5, C5-6: check lower cervical and upper thoracic mobility first.
Overhead athletes: train thoracic extension/rotation proactively, before pain appears.
CLOSING PRINCIPLE
This isn’t purely a strength problem or an aging problem. It’s a distribution problem.
The body has remarkable capacity to share load across dozens of small joints. When habitual posture concentrates that load onto two or three segments instead, those segments wear down faster than they were built to.
Restoring distribution of movement through the thoracic spine may be one of the most direct mechanisms by which Pilates protects the neck, shoulders, and low back.
FREQUENTLY ASKED QUESTIONS
Does thoracic spine mobility affect shoulder pain?
Yes. The scapula cannot extend or rotate horizontally on its own — it relies on the thoracic spine to supply that movement during any overhead activity. When the thoracic spine is restricted, the shoulder joint compensates, which can lead to mechanical impingement and rotator cuff irritation over time.
Is spinal extension safe for someone with osteoporosis?
Yes — extension is generally the safe and recommended direction for thoracic mobilisation in osteoporosis, while spinal flexion under load is typically the movement to avoid. Supported extension exercises, such as those using a Spine Corrector or stacked therapy balls, can help restore upright posture without the risks associated with flexion-based movement.
What causes rotator cuff tears after age 50?
Rotator cuff tear prevalence rises with age, but the cause is considered multifactorial — degeneration, microtrauma, and reduced tissue healing capacity all contribute. This article proposes that restricted thoracic spine mobility is also a significant, often overlooked, mechanical contributor, since it forces the shoulder to absorb movement it wasn’t designed to handle alone. Importantly, many tears found on imaging are asymptomatic.
Why does my lower back hurt even though I have good core strength?
Lower back pain at the L4-5, L5-S1 level is often linked to limited thoracic spine mobility rather than core weakness alone. When the thoracic spine doesn’t move enough during daily activity, the lumbosacral junction compensates and absorbs disproportionate force — research has shown that improving thoracic mobility can reduce lumbosacral stress significantly, even in a single session.
Can Pilates help with neck and shoulder pain?
Pilates exercises that target thoracic spine mobility and segmental breathing — such as Swan, Mermaid, Roll Up, and Spine Twist — can help restore the distribution of movement across the spine. This may reduce the concentrated stress at the cervical spine and shoulder girdle that contributes to chronic pain and degeneration.
Move well. Teach well. Live well. Floletics